The 2-Minute Version
- Private practice has shrunk from 60% of U.S. physicians in 2012 to 42% in 2024 and the trend is continuing
- The compensation gap between private practice and hospital systems exists, but is small and shrinking
- The 70% test is a good framework for determining if a change is needed
The Dollar Math On average, about $37K/year separates single-specialty group physicians from hospital-employed peers (Doximity 2025 Physician Compensation Report). This difference isn't enough of a driver on it's own to justify private practice over hospital employment. The main drivers are less monetary considerations such as autonomy, consistency, and coworkers.
You're a year out from finishing residency...."Hospital employment or private practice?"
You're three years into your first attending job and starting to look around..."Hospital employment or private practice?"
You're sitting across from a senior partner who just slid a buy-in number across the table...."Hospital employment or private practice?"
There's no clean answer and neither side wins on its own merits. The right call depends on how each path's trade-offs line up with your goals.
The Setup
In 2012, about 60% of U.S. physicians worked in physician-owned private practices. By 2024, that number shrunk to 42% and today it is even lower. Over the same time period, the share of physicians working in hospital positions grew from 29% to 47%. By 2024, hospital-affiliated employment had overtaken private practice for the first time, and the trend is going to continue into the future. (AMA 2024 Physician Practice Benchmark Survey)
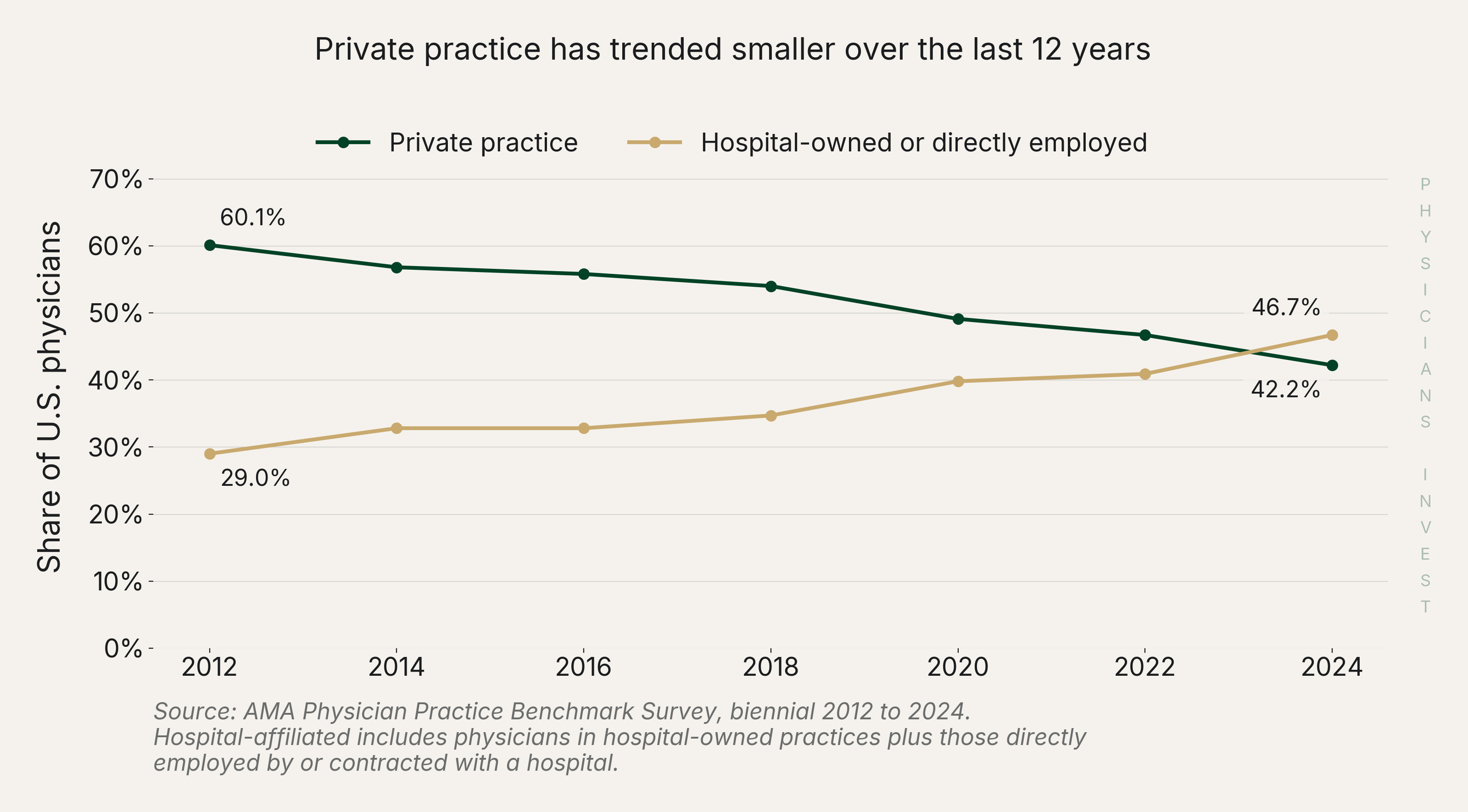 Source: AMA Physician Practice Benchmark Survey, biennial 2012 to 2024.
Source: AMA Physician Practice Benchmark Survey, biennial 2012 to 2024.
This trend matters for two reasons.
- It means the world has changed and old advice is most likely stagnant in this new hospital-heavy employment regime. Hospitals have been willing to pay more for physicians than they used to in order to fuel their growth.
- It means both options are still viable. 42% private practice is still tens of thousands of physicians.
The Analysis
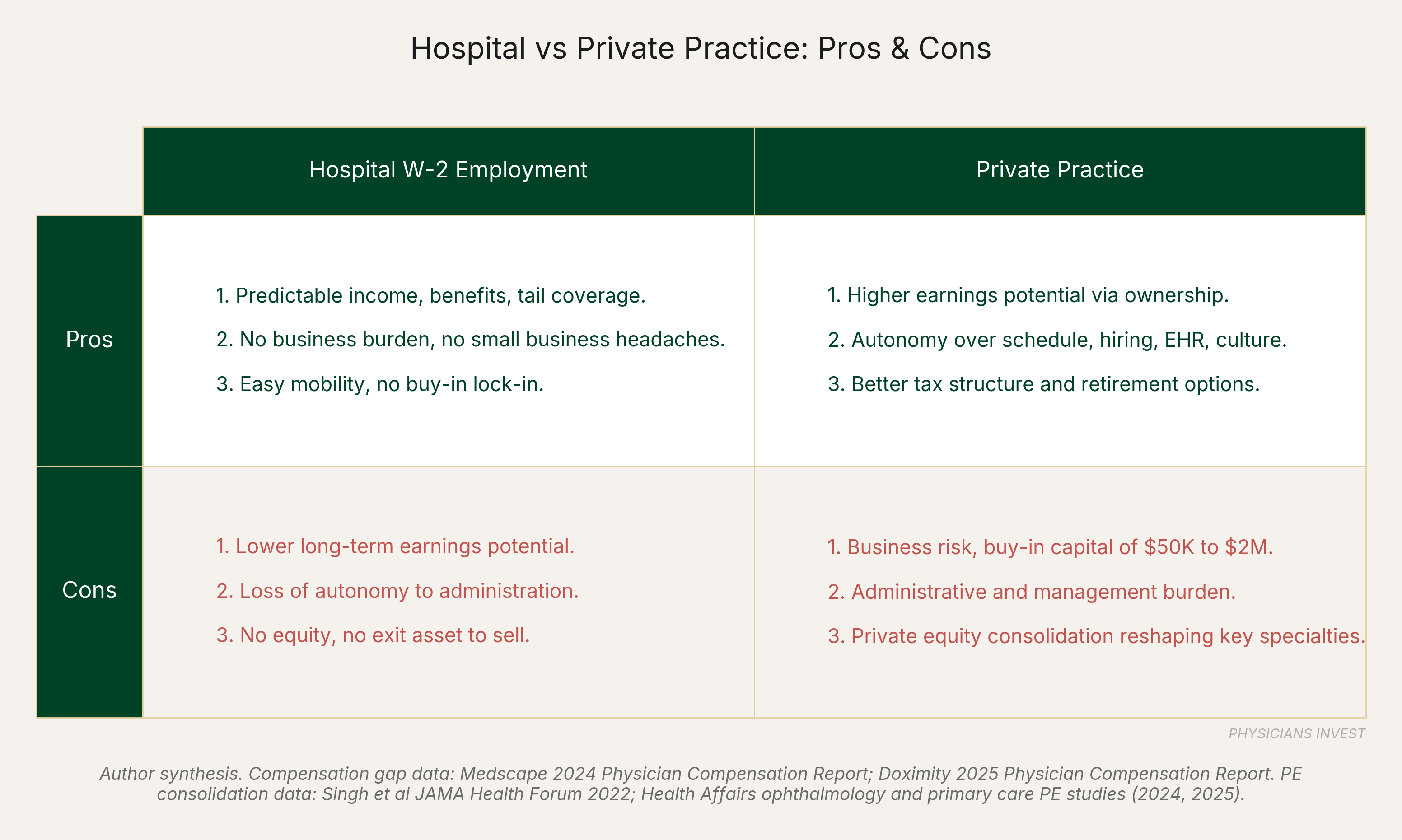
Two paths, Pros and Cons of Each
What you gain on one side is roughly what you give up on the other.
- Predictable income and full benefits vs higher earnings potential and autonomy
- No business burdens vs small business headaches
- Easy mobility vs established client base
The table below outlines the top 3 pros and cons for each path:
Hidden Downsides of Each Path
Choosing your people: So much of your enjoyment in your career is due to the people you're working with and around. In a large hospital system, you have very little say over who you work with. It's often assigned. Suboptimal teammates aren't fixable from your end, and the daily relational friction compounds. This is a huge advantage of private practice.
Small Business Pain Points: For private practice, the frustrations and anxiety that come with small businesses never go away. A small business is a more "eat what you kill" environment than hospital systems. The upside through equity is huge if you have a pathway to becoming a partner, but the partner path requires you to give up significant amounts of your time off.
Don't private practice physicians make a lot more money?
The salary gap isn't as large as you might think. The Doximity 2025 Physician Compensation Report puts single-specialty group physicians at an average of $476,807 and hospital-employed physicians at $439,319. That's about $37K a year. The main gap to be focused on isn't salary but in equity ownership and the upside that comes from that stake. The other lever that private practice physicians have is tax advantages if they are partners or 1099 contractors. The details of this are deep and we are reserving that topic for a future issue focused just on small business tax advantages.
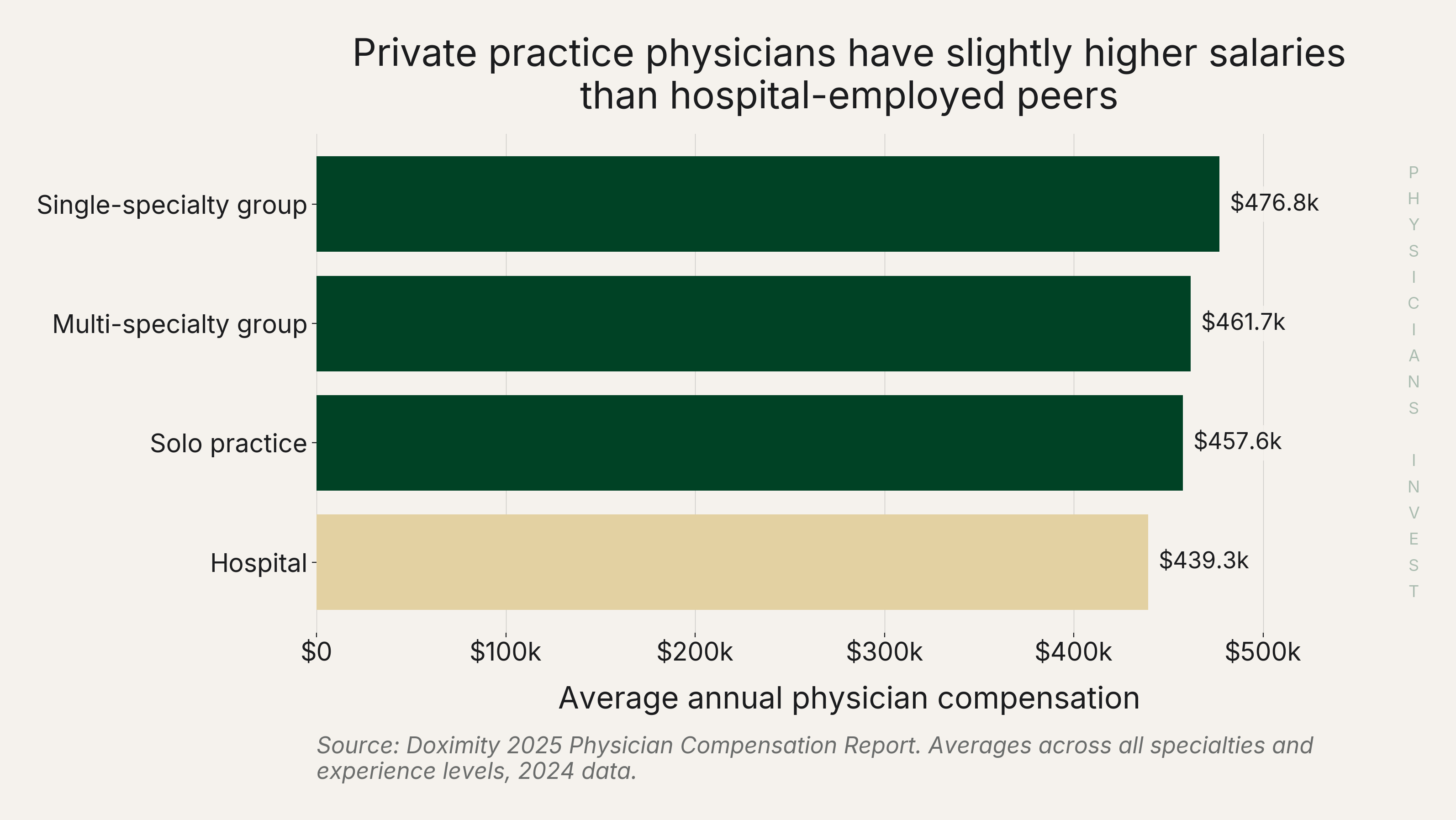 Source: Doximity 2025 Physician Compensation Report.
Source: Doximity 2025 Physician Compensation Report.
Where does private equity fit into this?
Private equity has a growing presence in private practice healthcare, and their focus is specialty-specific. 6.5% is the all-physician national average for the percentage of physicians working in private equity, up from 4.5% in 2022. This number seems small but it continues to grow. We would expect private equity ownership to increase across the sub-specialties they're focused on over the next decade. For physicians, it is important to learn about the private equity partner backing a private practice if you are considering working for one. Some private equity firms are great partners while others can create a miserable environment for both the patient and the physician.
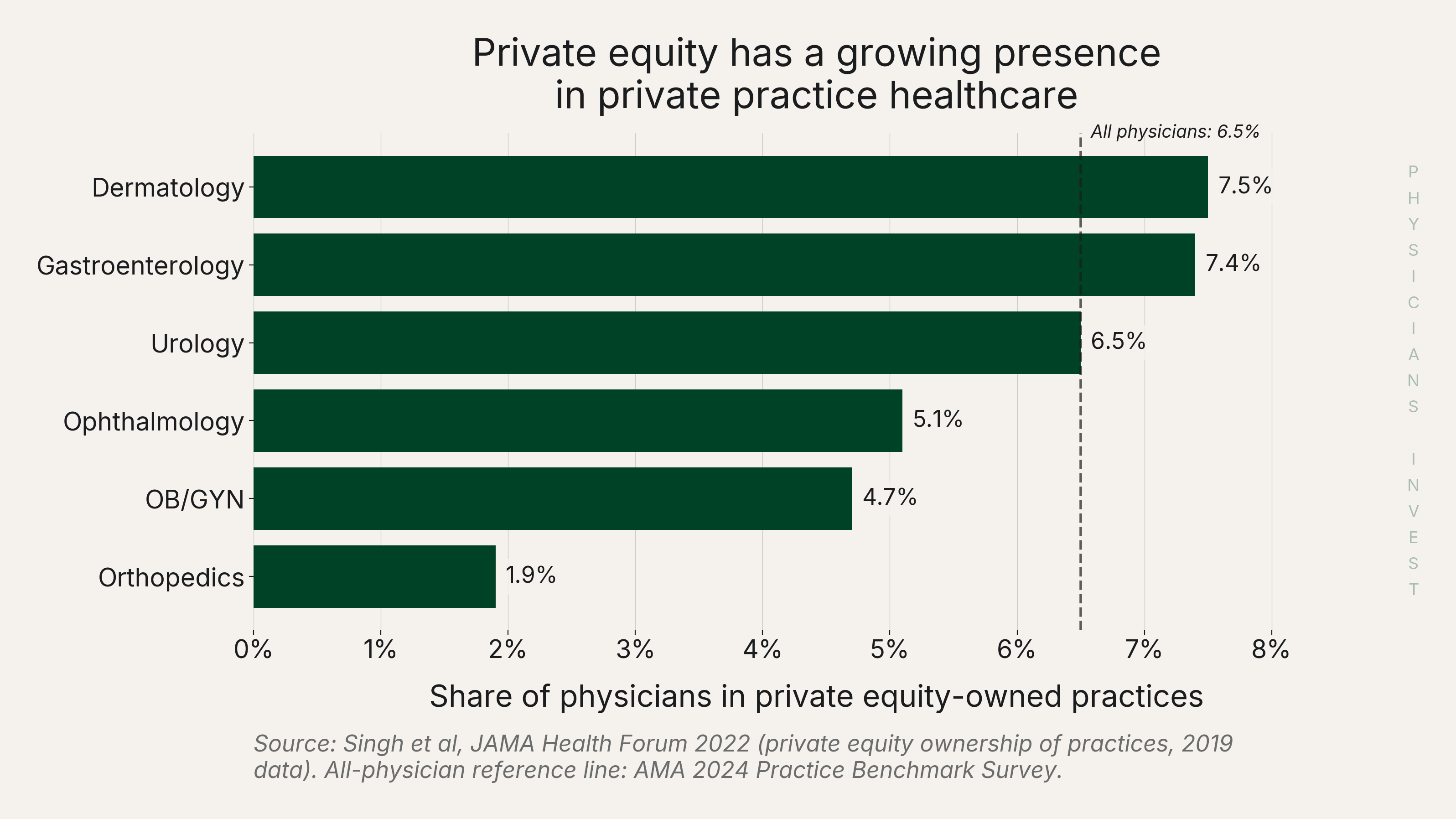 Source: Singh et al, JAMA Health Forum 2022; AMA 2024 Practice Benchmark Survey.
Source: Singh et al, JAMA Health Forum 2022; AMA 2024 Practice Benchmark Survey.
The Move
First: take the 70% test
If you're considering a jump, this question can help.
"Are you happy with your job 70% or more of the time?" Or said another way: "Do 70% or more of the things you do in your role bring you fulfillment?"
Every job has frustrations. The grass is always greener until you step on the other side and realize it's only because it was planted on top of a septic tank. The expectation that you should be happy 90% or 100% of the time at work is a modern trap.
If your answer is "yes", stay where you are and try to be the best version of yourself in that role. If "no", the change isn't necessarily flipping hospital to private practice or vice versa. It might be a lateral move: a different hospital system in your city or a different private practice with better owners. Be specific about what's not working for you before you decide what to change. We think of job jumping similar to surgery: it often fixes the main problem but it may introduce new ones.
Second: get equity exposure
Whichever path you're on, make sure you have equity exposure somewhere. Private practice with partnership opportunities gives it to you by default and is a great path for many physicians to consider. W-2 hospital employment caps your upside in the system itself, so you need to build equity outside the practice. Examples of how this could be done include real estate, concentrated stock exposures, a side business, small business investments, and mineral rights. Most physicians, both hospital and private practice employed, should seek significant long-term equity exposures.
We think equity ownership is the true wealth variable over a career. Salary should become noise at a certain point in your career. Whether you're W-2 at a hospital or a private practice partner, the question is the same: where is your equity?
Sources
Data
- AMA Physician Practice Benchmark Survey 2024 — physician employment and ownership trend data 2012-2024
- AMA Physician Practice Characteristics 2024 (PDF) — PE penetration by specialty and detailed ownership breakdowns
- Doximity 2025 Physician Compensation Report — compensation by practice setting (single-specialty group vs hospital)
- Medscape 2024 Physician Compensation Report (via Becker's) — self-employed vs employed physician pay comparison
Analysis
- Physicians Advocacy Institute / Avalere Study on Physician Employment Trends 2019-2023 — hospital vs corporate ownership crossover; 77.6% employed figure
- Singh et al, "Geographic Variation in Private Equity Penetration Across Physician Specialties," JAMA Health Forum 2022 — PE penetration rates by specialty used in chart
- Health Affairs: Physician Turnover Increased in PE-Acquired Practices (2024) — ophthalmology turnover data post PE acquisition
- Physician Side Gigs: Partnership Pathways for Private Practice — partnership track models and typical buy-in ranges