The 2-Minute Version
- 78% of physicians sign their employment contract without an attorney review. The average review costs $480 to $1,500 and typically uncovers $20K to $50K in unaddressed compensation.
- Where you work determines whether you're handcuffed more than where you live. Non-compete prevalence runs from 0% (active duty) to 79% (PE-backed group practice).
- Nine states reformed physician non-competes in 2024-2026, but nearly all reforms are prospective only. This means they protect the next contract, not the one you already signed.
- Bring 10 rules to your next contract negotiation. We cover 6 things to always do and 4 to never do.
No one enjoys reading legal contracts but it's a necessary evil and physicians must learn to play the game. Here's a story of how a physician lost $155,000 from a contract review overlook.
True story. An Arizona physician's contract measured the non-compete radius from any facility in a large health system, not from where they actually practiced. The clause locked them out of all of Phoenix and forced an interstate move. The associated damage: $15K in moving costs, roughly $50K in carrying costs on a home that sat for six months, $20K in closing on the new house, and a $70K realtor fee on the old one. The realtor fee on the first home alone exceeded most physicians' signing bonuses. All from one line an attorney would have flagged in fifteen minutes and the HR department would have most likely agreed to on the front end. That damage was avoidable.
Below is an article on the best rules to follow when negotiating your next contract. Don't share this with employers.
The Setup
Legal documents are scary and negotiations aren't fun for anyone. Further, physicians are time-constrained and because of that most physicians don't put in enough time to get the initial contract right. It's estimated that 78% (per AMA data) never have an attorney review their contract before signing. From our research of 2026 industry pricing (Contract Diagnostics, Contract Rx, Resolve), the average review costs $480 to $1,500 and the average value found is $20,000 to $50,000. That's a return on investment (ROI) of 10x to 100x, and well worth doing.
Many physicians think the negotiations happen during the interviews but the true negotiation is after the contract has been received. The contract drives the negotiation. Salary, signing bonus, and clauses are all on the table at once. Be the physician who pushes on all three. We know it feels awkward, but these HR departments expect it.
This is also the moment you have the most leverage you'll ever have with the employer and it's important to capitalize on that. They've already decided they want you because the offer is in writing. They're trying to close just like a realtor would try to close a house and are willing to push to make concessions. Once you've signed, your leverage is gone, and the next renegotiation is two or three years away. By then you're the incumbent and it can make negotiations feel even more awkward than if they happened on the front end. The rule here is: use the leverage while you have it.
As one physician we work with put it: "Things are always bright and sunny on the front end with employment. It's the back end that you have to worry about." So what are the practical things to pursue on the front end?
Where the Dollars Hide
Non-competes: Non-competes are an "employer-type problem" more than they are a "state problem". Prevalence of an included non-compete in your contract runs from 0% (active duty military) to 79% (PE-backed group private practice). Of course private equity is the worst offender here. Physicians in non-academic systems sit at 64%. The state law doesn't matter much if your employer doesn't include a non-compete to begin with. The chart below shows the breakdown by employer type.
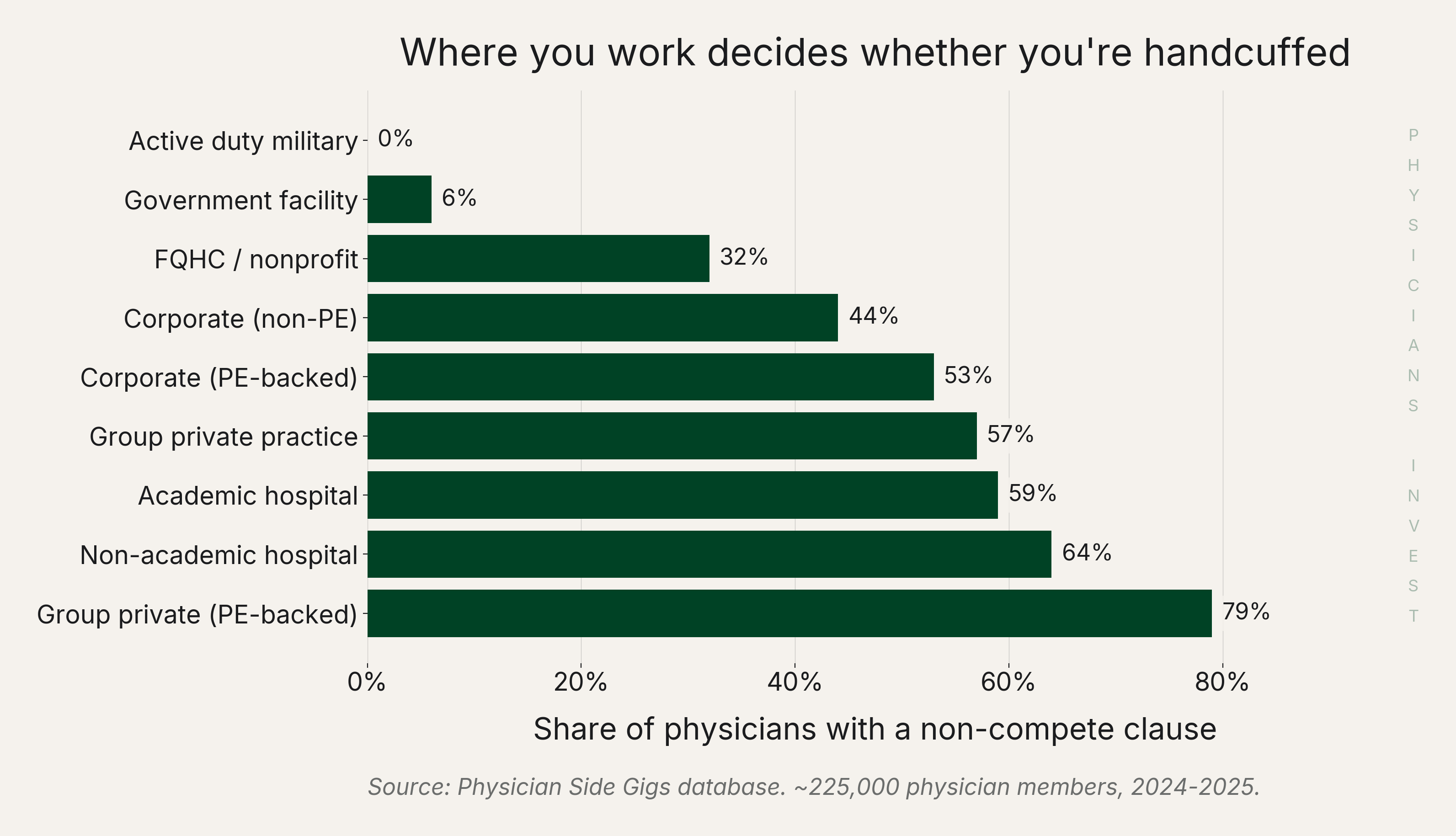 Source: Physician Side Gigs database, 2024-2025.
Source: Physician Side Gigs database, 2024-2025.
Tail Coverage: This could be a huge bill on your way out. Most physicians carry "claims-made" malpractice insurance (the cheaper form for employed physicians; "occurrence" policies are mostly academic medicine). Claims-made covers you only when both the alleged event AND the filed claim happen while the policy is active. The day you leave, coverage stops. But malpractice claims routinely surface years after the patient encounter. Tail coverage is the one-time lump-sum premium that buys continued reporting protection, priced at 150% to 300% of your last annual premium. To put some numbers to it, Family medicine is roughly $19K and OB/GYN in a high-risk state is roughly $305K. If your contract says "physician shall be responsible for tail coverage" and you sign, that's a six-figure mistake for some specialties. Read the assignment before you sign anything. Average tail premiums by specialty are below.
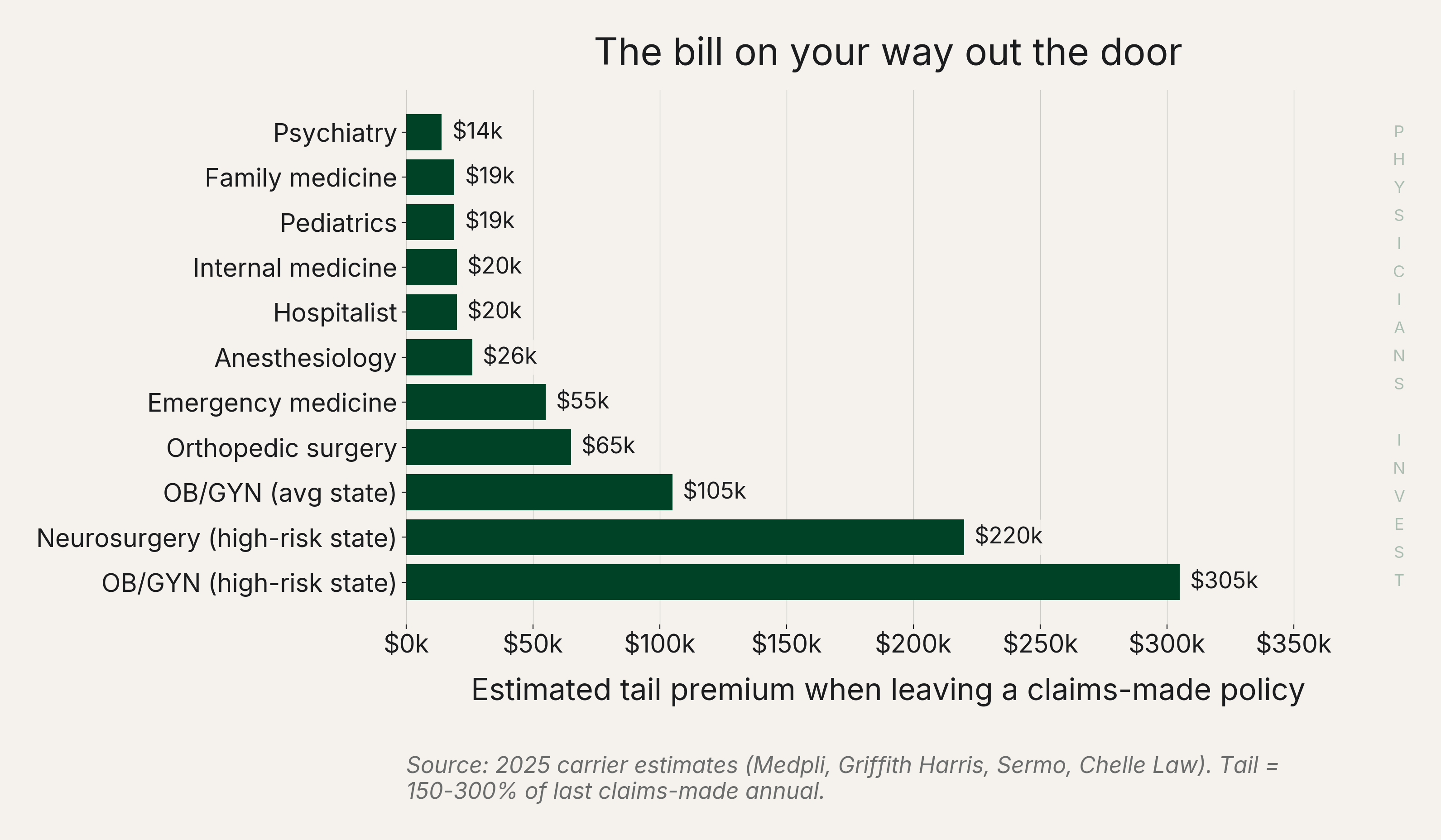 Source: 2025 carrier estimates (Medpli, Griffith Harris, Sermo, Chelle Law).
Source: 2025 carrier estimates (Medpli, Griffith Harris, Sermo, Chelle Law).
Signing Bonus: Good news...the 2025 average is $38,215, up 23% from 2024 (see chart below). But remember, the negotiation for your signing bonus is more than the headline number. It's the claw-back too. Most contracts use 2-4 year prorated forgiveness. The issue is that when you receive your signing bonus, you pay tax that year but aren't fully vested in the money until years later. If you leave early and repay the bonus you are still out the tax you already paid. Fortunately, federal Section 1341 lets you recover the federal tax on the original payment. BUT your state tax may be stranded. Pennsylvania is the main one to worry about as it has no §1341 equivalent. California, New York, Illinois, and Ohio do allow claw-backs. Texas and Florida have no state income tax to recover. State tax treatment varies by individual circumstance. Confirm with a tax professional before relying on our word here.
Most physicians don't fight hard for either an increase in salary or their signing bonus. Play the game and treat both as live numbers. A good resource on this is Never Split the Difference by Chris Voss, the FBI hostage negotiator turned negotiation coach.
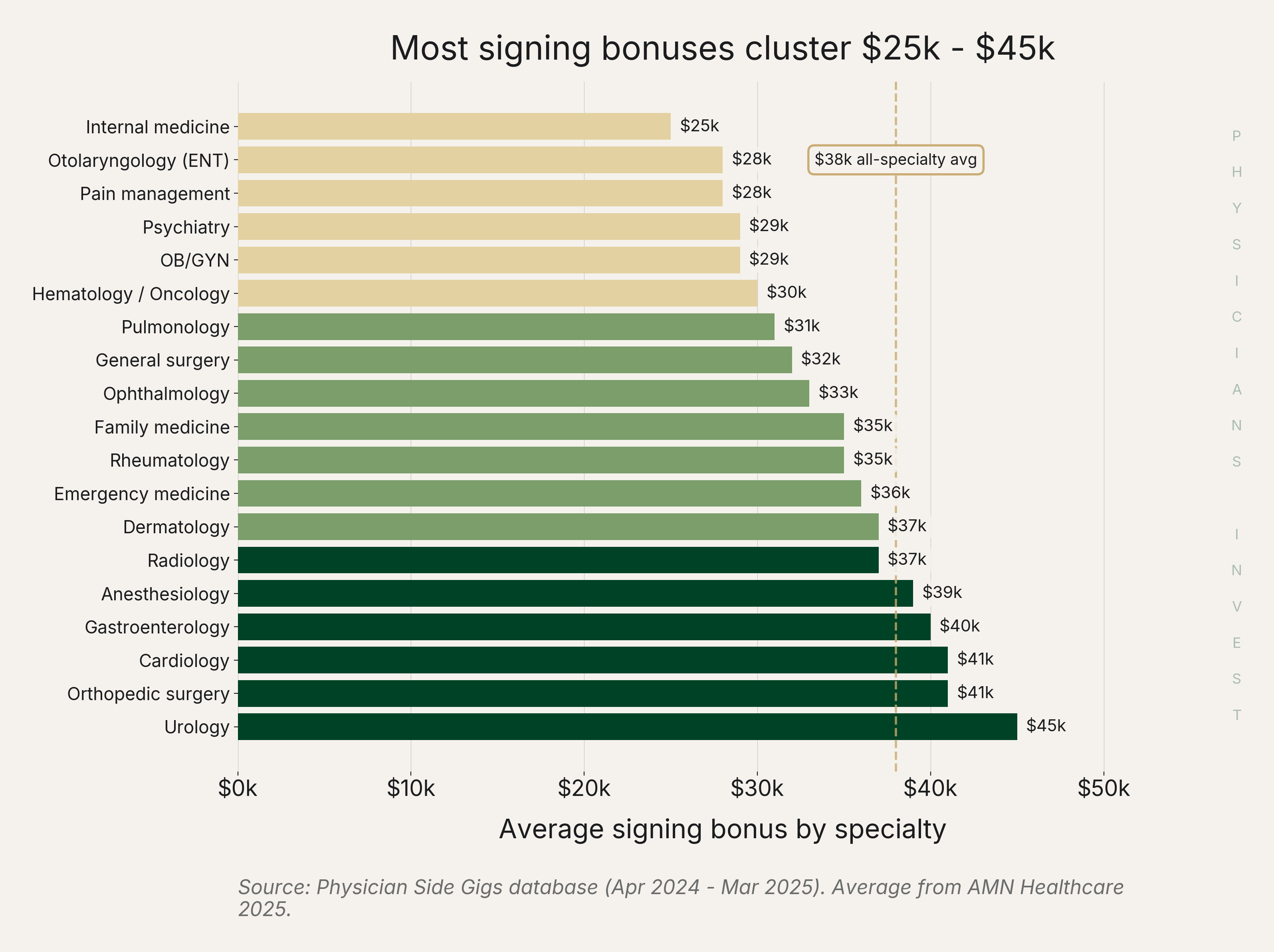 Source: Physician Side Gigs database (Apr 2024 - Mar 2025). Average from AMN Healthcare 2025.
Source: Physician Side Gigs database (Apr 2024 - Mar 2025). Average from AMN Healthcare 2025.
The Less Common Ones: Three more clauses are worth serious money but get less attention than they deserve.
- (1) Without-cause termination is in 97% of physician contracts. The notice term should be symmetric or, ideally, asymmetric in your favor, with a clause that voids the non-compete if the employer terminates without cause. An example of this is that if they require you to give 90 day notice, they have to give 90 day notice.
- (2) wRVU floors (work relative value units, the productivity metric most physician compensation formulas are built on) with fixed-dollar conversion factors lose value to inflation over time. CMS (the Centers for Medicare & Medicaid Services, the federal agency that sets Medicare reimbursement) finalized a -2.5% efficiency adjustment on wRVUs for non-time-based services in 2026, which mechanically suppresses procedural wRVUs on contracts using fixed-multiplier formulas.
- (3) Non-solicit clauses are often broader than the non-compete, survive longer, and become the de-facto non-compete in states that ban the real one. It's unlikely they remove their non-solicit clause but make sure the terms are reasonable.
State Rules Still Matter
Which state you practice in matters just as much as your employer type. Lots of change has happened with non-competes over the last couple years and here is a breakdown.
Nine states reformed physician non-competes in 2024-2026. Texas SB 1318 caps physician non-competes at five miles and one year and voids them if the employer fires the physician without cause. Pennsylvania HB 1633 caps at one year. Indiana SEA 475 banned hospital-physician non-competes outright. Four total-ban states: California, Minnesota, Oklahoma, North Dakota. The graphic below is accurate as of April 2026.
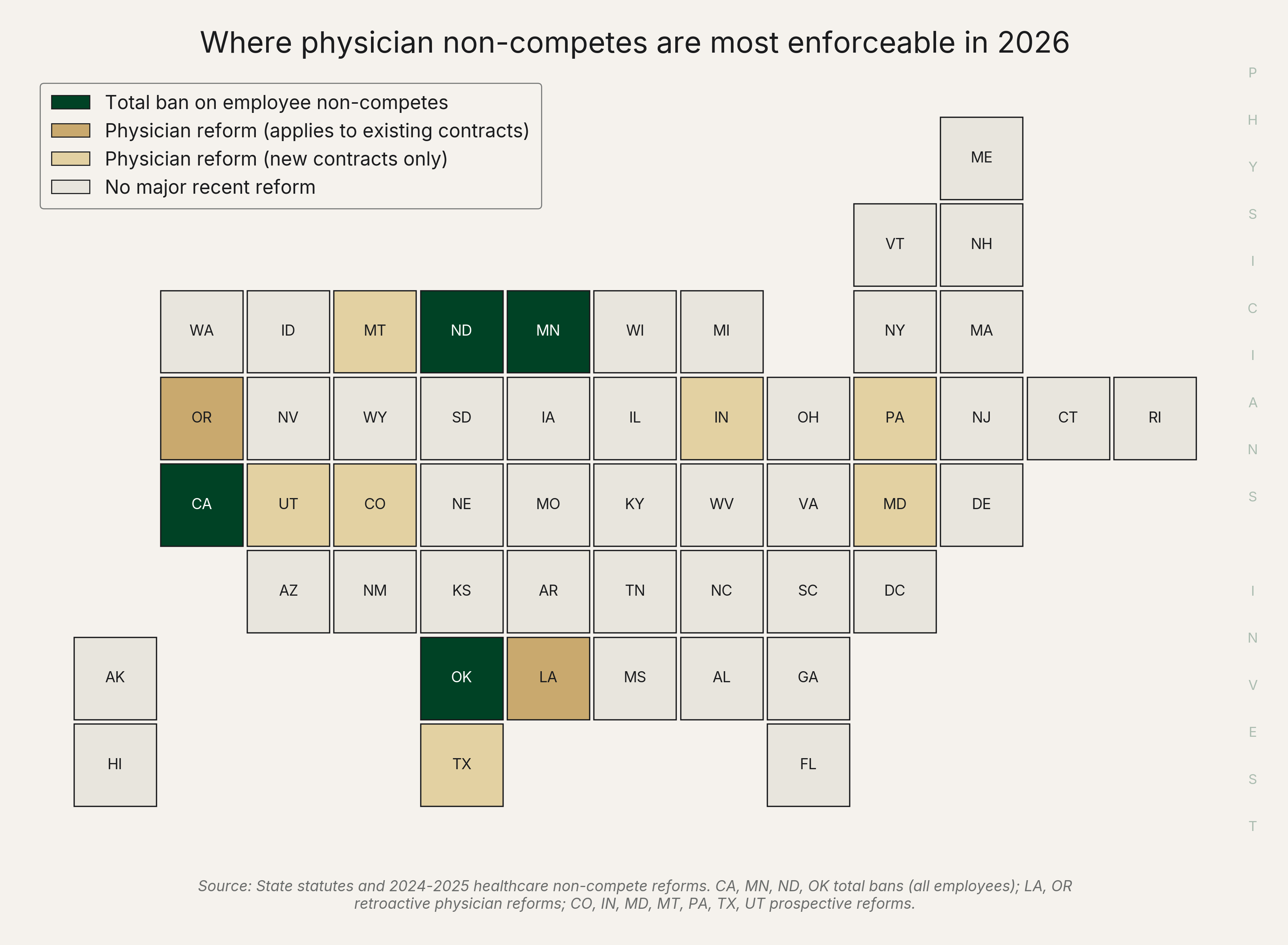 Source: State statutes and 2024-2025 healthcare non-compete reforms.
Source: State statutes and 2024-2025 healthcare non-compete reforms.
There is some bad news with all this state-law reform...almost every reform is prospective only. Only Oregon (HB 3410) and Louisiana have any retroactive reach. For example, even though Texas made favorable changes, a physician in Texas under a 2023 non-compete is still bound by pre-SB 1318 enforceability. The reforms protect the next contract, not the one you already signed in most states.
The seven largest physician-employed states (California, New York, Texas, Florida, Pennsylvania, Illinois, Ohio) cover the majority of practicing physicians. Of those, only California (long-standing total ban), Texas (SB 1318), and Pennsylvania (HB 1633) have modern physician non-compete reform. Rudely, Florida's 2025 broader reform expressly excluded healthcare. New York, Illinois, and Ohio still operate in the stone-ages under general reasonableness review.
| State | Physician non-compete | Retroactive? | State §1341 equivalent? |
|---|---|---|---|
| California | Total ban (all employees) | — | Yes (Schedule CA Pt II) |
| New York | General reasonableness | — | Yes (Form IT-257 credit) |
| Texas | 5-mile, 1-year cap (SB 1318) | New contracts only | No state income tax |
| Florida | Tight enforcement (no carve-out) | — | No state income tax |
| Pennsylvania | 1-year cap (HB 1633) | New contracts only | Limited / unclear |
| Illinois | General reasonableness | — | Yes (statutory) |
| Ohio | General reasonableness | — | Yes (statutory) |
Source: State statutes; AAMC/KFF physician headcounts; state revenue codes for §1341 equivalents (April 2026).
So what do physicians need to do about all this?
The Move
We've drafted 10 rules for any physician about to sign a contract. 6 things to always do. 4 to never do.
Always do:
- Pay for an attorney review. $480 to $1,500. The best ROI you'll find out there.
- Negotiate the salary AND the signing bonus on top of every clause. The contract is more of a negotiation than the offer.
- Fight for asymmetric without-cause notice in your favor. Opening ask: 90+ days from the employer, 30 from you. They're a system built to absorb a departure. You have a family, a lease or mortgage, and credentialing timelines that take months. Symmetric notice is the fallback. Asymmetric notice flipped against you (employer 30 days, physician 180+) is a walk.
- Require the non-compete and the non-solicit to be void if the employer terminates you without cause.
- Know who pays the tail insurance in writing. Not "we'll figure it out."
- Demand a "cause" definition with a cure period. "Cause" without a cure period is firing-at-will in disguise. An attorney can help with this.
Never do:
- Never sign within 3 days of receiving. Pressure tactics are a red flag. It is often recommended to wait until a day or two before the deadline.
- Never accept a non-compete radius measured from "system-wide" facilities. The Arizona story at the beginning of this article shows the damage that clause does.
- Never accept a fixed-dollar wRVU rate without an annual escalator. Inflation is built into our economic system and your rate should keep up.
- Never trust a "partnership track" promise without a written buy-in formula. "Partnership" can mean book value, FMV, or nothing at all.
Overall, when it comes to contract negotiation the little details matter and they add up. Things are always bright and sunny on the front end of contracts which means that is the best time to get things right. Otherwise, the back end could be miserable.
Sources
Data
- Physician Side Gigs: Physician Non-Compete Clause Database -- non-compete prevalence by employer type
- AMN Healthcare 2025 Physician & AP Recruiting Incentives Report -- signing bonus average and year-over-year change
- MGMA 2025 Provider Compensation Report -- wRVU benchmarks
Policy
- AMA: Finding a Lawyer to Review Your Physician Employment Contract -- 78% attorney-review statistic
- Bradley: Texas SB 1318 Analysis -- Texas non-compete caps and void-on-termination provision
- Morgan Lewis: Pennsylvania HB 1633 -- Pennsylvania one-year cap
- Foley: Indiana Physician Non-Compete Ban 2025 -- Indiana SEA 475 hospital-physician ban
- Barran Liebman: Oregon HB 3410 -- Oregon retroactive non-compete reform
- CMS 2026 Medicare Physician Fee Schedule Final Rule -- wRVU efficiency adjustment
- MGMA: 2026 Work RVU Efficiency Adjustment -- specialty-level wRVU impact analysis
Industry
- Contract Diagnostics -- 97% without-cause prevalence; $20K-$50K value-found range
- Medpli: Physician's Guide to Tail Insurance -- tail coverage pricing and claims-made mechanics
- Griffith Harris: Average Cost of Tail Insurance -- specialty tail premium ranges
- Physicians Thrive: Contract Review -- 48-72 hour pressure tactic red flag; value-found corroboration
Tax
- The Tax Adviser: Section 1341 Claim of Right -- federal §1341 mechanics
- NY Dept. of Taxation: Form IT-257 Claim of Right Credit -- New York §1341 equivalent